
Fall Detection vs. Fall Prediction: Why Preemptive Fall Prevention Matters


Fall detection vs fall prediction is an important distinction in hospital fall prevention because each category solves a different timing problem. Fall detection alerts after a fall has occurred or may already be underway. Fall prediction identifies patients at elevated risk. Preemptive fall prevention alerts earlier, when a vulnerable patient shows intent to sit up from a lying position. For patient safety leaders and clinical executives, defining the “alert window” around sit-up intent can support safer mobility, earlier intervention, and strengthen existing fall-prevention protocols.
Methodology note: This article is informed by 14 exploratory calls with healthcare leaders, clinicians, and patient safety stakeholders, along with my perspective as a former Mechanical Engineering professor and founder developing the OK2StandUP System and OK2Predict AI service layer.
A Practical Framework: Fall Detection vs. Fall Prediction vs. Preemptive Fall Prevention
Hospitals often use the terms fall detection, fall prediction, and fall prevention as if they mean the same thing. They do not.
The difference is timing.
For healthcare leaders, the practical question is not only whether a technology can identify risk or send an alert. The more important question is whether the system creates an actionable window for nurses or aides to intervene before a vulnerable patient is upright, unassisted, and at risk of falling.
That timing distinction is especially important because many inpatient falls occur during predictable mobility events — when patients attempt to sit up, stand, transfer, toilet, or walk without assistance. Dr. Eileen Hitocho of Washington University School of Medicine, found that 85% of inpatient falls occurred in the patient’s room, 79% were unassisted, and 50% were elimination-related1.
In the sections that follow, we break down three categories of fall-related technology: fall detection, fall prediction, and preemptive fall prevention. Each plays a different role in hospital patient safety. But their value depends on where they operate in the fall-risk timeline — after a fall, before a future risk period, or during the short bedside mobility window when intervention may still be possible.
Fall detection vs. fall prediction vs. preemptive fall prevention
What is Fall Detection
Fall detection is technology that identifies when a patient fall has occurred or when movement data suggests that a fall may have taken place.
In hospitals and long-term care facilities, the purpose is straightforward: notify staff so they can respond, assess the patient, document the event, and escalate care when needed. In some workflows, alerts go directly to bedside staff. In others, a centralized observer, virtual sitter, or monitoring team may review the alert before dispatching point-of-care nurses or aides.
Patient fall detection technologies may include bed- or chair-based sensors, wearable devices, smart beds, room sensors, cameras, radar, accelerometers, or other monitoring tools. These systems may detect sudden impact, abnormal motion, body position changes, prolonged inactivity, or other signals that suggest a fall event.
That function has real value. Fall detection can support faster response, post-fall assessment, documentation, root-cause review, quality reporting, and care escalation.
Its primary limitation is timing.
In practical terms, fall detection answers:
“Has the patient already fallen, or is there evidence that a fall may have occurred?”
That question matters for response and reporting. But for hospitals trying to reduce inpatient falls, fall-related injuries, length of stay, liability exposure, and reimbursement risk, fall detection alone has a clear limitation: it usually alerts after the event is underway or after it has already happened.
Key takeaway: Fall detection helps hospitals respond after a suspected fall event. Its value is faster response and documentation, but its limitation is timing: it usually alerts after the fall is underway or has already happened.
What is Fall Prediction
Fall prediction is the process of estimating which patients are more likely to fall based on clinical risk factors, functional status, mobility limitations, medications, cognition, prior falls, toileting needs, balance, gait, or changes in condition.
Unlike fall detection, which focuses on whether a fall may have already occurred, fall prediction looks forward. In practical terms, fall prediction answers:
“Who is likely to fall?”
But fall prediction can operate across different time horizons.
· Long-horizon fall prevention focuses on reducing baseline fall risk over weeks, months, or years. These strategies may include evidence-based interventions such as balance training, strength exercise, gait support, medication review, vision assessment, footwear assessment, environmental modification, mobility support, and patient education.
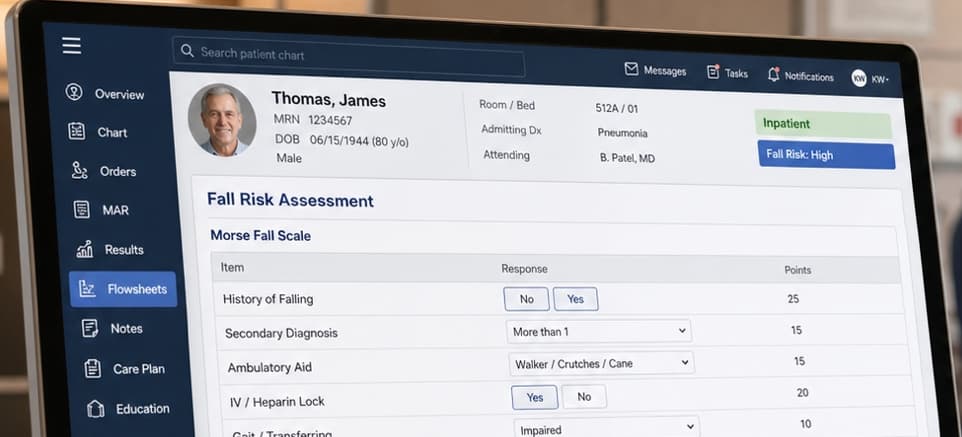
· Episode-level fall prediction focuses on identifying which patients are at elevated risk during an admission. In hospital fall prevention, a fall risk assessment helps care teams assess and document patient-specific risk factors. Tools such as the Morse Fall Scale2 and STRATIFY3 help care teams assess and document fall risk, while evidence-based programs such as Fall TIPS4 — developed through an AHRQ Patient Safety Learning Lab — translate that risk assessment into a patient-specific fall prevention plan.
· Immediate-horizon fall prevention focuses on the near-real-time window when a vulnerable patient may be beginning a movement sequence that requires help now. This is different from classifying a patient as high risk. It asks whether the patient is starting to sit up, stand, transfer, toilet, or walk without assistance.
Fall prediction helps answer:
“Who is likely to fall?”
Immediate-horizon fall prevention asks a more time-sensitive question:
“Is the patient beginning a movement sequence that requires help now?”
Key takeaway: Fall prediction helps hospitals identify patients at elevated risk and plan preventive care. Its value is risk stratification and tailored intervention planning, but its limitation is timing: it may identify who is at risk without telling the care team when unsafe movement is beginning.
What is Preemptive Fall Prevention?

Preemptive fall prevention focuses on the immediate horizon: the short window when a vulnerable patient begins moving in a way that may require staff intervention now.
Unlike fall detection, which asks whether a fall has already happened, and fall prediction, which asks who is likely to fall, preemptive fall prevention asks:
“Is the patient beginning a movement sequence that requires help now?”
In a hospital room, that movement sequence may begin before the patient is standing, transferring, toileting, or walking. For many vulnerable patients, the risk sequence can start when they begin moving from lying down toward sitting up at the edge of the bed.
This matters because getting out of bed is not instant. Bed mobility research shows that the time required to move from lying down to sitting can vary significantly by patient population. Neil B. Alexander, an MD and Professor of Internal Medicine at the University of Michigan Institute of Gerontology, did extensive research on this topic.5 His research shows that the time required to rise from bed increases substantially across older and more functionally vulnerable populations.
These data show why the alert window is not the same for every patient population. More vulnerable patients may have a longer bedside mobility transition, which may create a meaningful window for earlier intervention.
Time it takes to transition from supine to sitting at the edge of a bed.
The core question for preemptive fall prevention is:
Can technology recognize sit-up intent early enough to create an actionable alert window for nurses or aides?
The goal is not simply to classify a patient as high risk or respond after a fall. The goal is to identify earlier bedside movement signals — especially sit-up intent from a lying position — so the care team may have time to intervene before unsafe mobility progresses.
Key takeaway: Preemptive fall prevention focuses on the immediate-horizon movement window. Its value is creating an earlier alert when a vulnerable patient shows sit-up intent from a lying position, before the patient attempts an unassisted bed exit, transfer, or ambulation.
Final Takeaway: Timing Defines the Category
Fall detection, fall prediction, and preemptive fall prevention are all part of a hospital fall-prevention strategy, but they do not solve the same problem.
Fall detection helps care teams respond after a fall may have occurred.
Fall prediction helps hospitals identify which patients are at elevated risk.
Preemptive fall prevention focuses on the immediate-horizon movement window, when a vulnerable patient shows sit-up intent from a lying position and may need help now.
For clinicians, the distinction matters because reducing inpatient falls is not only about knowing who is at risk. It is about whether the care team receives an actionable signal early enough to intervene before unsafe mobility progresses.
The better evaluation question is:
Does the alert arrive early enough for nurses or aides to act?
As hospitals move from reactive monitoring toward earlier intervention, preemptive fall prevention may become an important part of a more proactive patient safety strategy.
For a deeper look at this shift, read our pillar article on preemptive AI patient safety monitoring.
FAQ
What is the difference between fall detection and fall prediction?
Fall detection identifies when a fall has occurred or may already be underway. Fall prediction identifies which patients are more likely to fall based on risk factors such as prior falls, mobility limitations, medications, cognition, toileting needs, balance, gait, or changes in condition. The main difference is timing: detection focuses on response after a suspected event, while prediction focuses on identifying risk before an event occurs.
What is the difference between fall prediction and preemptive fall prevention?
Fall prediction helps identify who is at risk. Preemptive fall prevention focuses on when a patient may need help now. For example, a patient may be classified as high risk at admission, but that does not tell the care team when the patient is beginning to sit up, stand, transfer, or walk without assistance.
What is preemptive fall prevention?
Preemptive fall prevention focuses on the immediate-horizon movement window when a vulnerable patient begins moving in a way that may require staff intervention. In this article, that window is centered around sit-up intent from a lying position, before the patient attempts an unassisted bed exit, transfer, or ambulation.
Why does sit-up intent matter in hospital fall prevention?
Sit-up intent matters because many unsafe mobility events begin before a patient is standing or walking. For vulnerable patients, the risk sequence may begin when they start moving from lying down toward sitting at the edge of the bed. Identifying that movement earlier may give nurses or aides a short window to intervene before unsafe mobility progresses.
What should hospitals ask when evaluating fall-prevention technology?
Hospitals should ask: Does the alert arrive early enough for nurses or aides to act? The question is not only whether a system detects movement, identifies risk, or sends an alert. The operational value depends on whether the alert creates enough lead time for staff to intervene before unsafe mobility progresses.
1. Hitcho EB, Krauss MJ, Birge S, et al. Characteristics and circumstances of falls in a hospital setting: a prospective analysis. Journal of General Internal Medicine. 2004;19(7):732–739. doi:10.1111/j.1525-1497.2004.30387.x.
2. Morse JM, Morse RM, Tylko SJ. Development of a scale to identify the fall-prone patient. Canadian Journal on Aging. 1989;8(4):366–377.
3. Oliver D, Britton M, Seed P, Martin FC, Hopper AH. Development and evaluation of evidence based risk assessment tool (STRATIFY) to predict which elderly inpatients will fall: case-control and cohort studies. BMJ. 1997;315:1049–1053. doi:10.1136/bmj.315.7115.1049.
4. Agency for Healthcare Research and Quality. Fall TIPS: A Patient-Centered Fall Prevention Toolkit. AHRQ states the toolkit was developed through an AHRQ Patient Safety Learning Lab and consists of a formal risk assessment and tailored plan of care for each patient.
5. Alexander, N. B., Grunawalt, J. C., Carlos, S., & Augustine, J. (2000). Bed mobility task performance in older adults. Journal of Rehabilitation Research and Development, 37(5), 633–638.
Related Blogs



Transform care through knowledge! Subscribe to our blog and keep up to date with advances in senior care.
We're committed to your privacy. OK2StandUP uses the information you provide to us to contact you about our relevant content, products, and services. You may unsubscribe from these communications at any time. For more information, check out our privacy policy.
